In Partnership with InvestorPlace
Medical Establishment Quietly Legalizes Organ Harvesting from Living Patients
Clear Facts
- Medical authorities have expanded protocols allowing organ harvesting from patients who have not suffered brain death, reclassifying cardiac death as sufficient grounds for organ removal
- The practice involves removing life support, waiting for the heart to stop, then quickly extracting organs while tissue remains viable—often within minutes of cardiac arrest
- Critics warn this creates financial incentives for hospitals and transplant centers to prematurely declare patients deceased, fundamentally altering the traditional definition of death
America’s medical establishment has quietly revolutionized the definition of death itself, opening the door to organ harvesting practices that would have been unthinkable just decades ago. What was once reserved only for brain-dead patients has now expanded to include anyone whose heart has stopped beating—even if brain function continues.
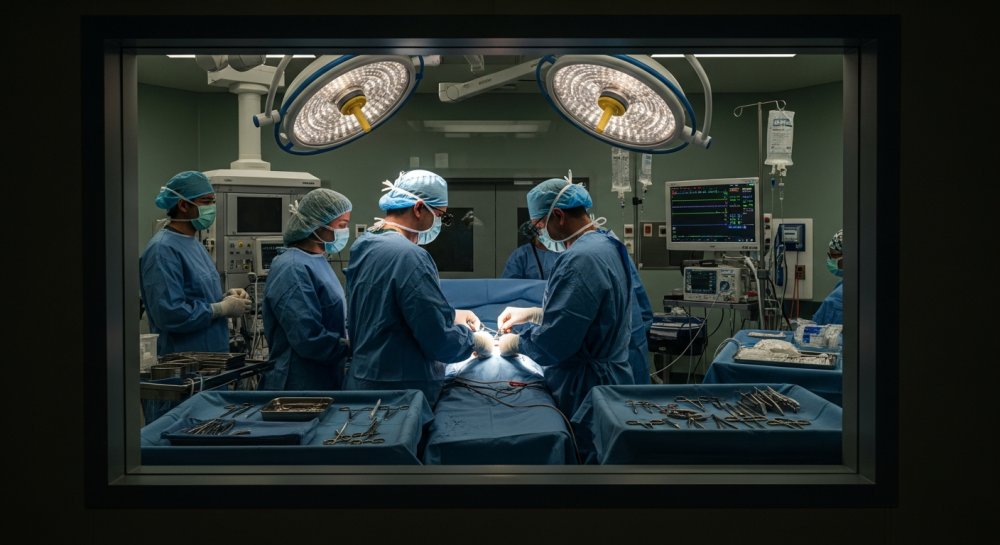
The new protocols, known as “donation after circulatory death” or DCD, allow doctors to remove life support from critically ill patients, wait for their hearts to stop, then rush them to operating rooms for organ extraction. The timeline is critical: organs must be harvested within minutes to remain viable for transplantation.
This isn’t a fringe practice. Major medical centers across the country have adopted DCD protocols, driven by the enormous demand for transplantable organs and the substantial revenue they generate. A single organ donor can provide tissue worth hundreds of thousands of dollars to the medical system.
The ethical concerns are staggering. Traditional medical ethics held that death occurs when the entire brain ceases to function—a clear, irreversible line. Now, hospitals are accepting cardiac death as sufficient, even though the brain may still be active and the heart could potentially be restarted.
<"The most urgent application of this is happening right now in operating rooms across America," one medical ethicist warned.
The timing raises questions about conflicts of interest. When hospitals know a patient is a potential organ donor, does that knowledge influence end-of-life care decisions? Do transplant coordinators have too much influence in determining when to withdraw life support?
Families facing the worst moments of their lives are often approached about organ donation before their loved one has even died. The pressure to consent can be overwhelming, especially when medical staff present donation as a way to find meaning in tragedy. Few families are informed about the controversial nature of DCD protocols or the debate within the medical community about whether these patients are truly deceased.
The financial incentives cannot be ignored. Transplant programs are highly profitable for hospitals, and organ procurement organizations operate with substantial budgets. While federal law prohibits buying and selling organs, the system surrounding organ transplantation generates billions of dollars annually.
Some medical professionals have raised alarms about the speed with which these protocols have been adopted. Unlike traditional brain death, which requires extensive testing and observation, cardiac death can be declared after just two to five minutes without a heartbeat. Critics argue this timeframe is arbitrary and potentially premature.
There’s also the matter of anesthesia. Some DCD protocols call for administering pain medication to organ donors before extraction, raising the disturbing question: if the patient is truly dead, why would pain relief be necessary?
The medical establishment has largely dismissed these concerns, insisting that current protocols are ethically sound and that DCD has saved countless lives through increased organ availability. They point to the thousands of patients waiting for transplants, many of whom will die before a suitable organ becomes available.
But the fundamental question remains: has the definition of death been changed to suit the needs of the transplant industry rather than to reflect biological reality? Are we harvesting organs from patients who might otherwise recover, or at minimum, deserve more time before being declared deceased?
The debate touches on core questions of medical ethics, the value of human life, and the point at which a person transitions from patient to organ source. As technology advances and the demand for organs continues to grow, these questions will only become more urgent.
Traditional conservatives have long warned about the dangers of utilitarian ethics in medicine—the idea that individual lives can be sacrificed for the “greater good.” The expansion of organ harvesting protocols represents exactly this kind of thinking: redefining death itself to maximize the number of available organs, regardless of the moral costs.
What happens when the incentive to obtain organs conflicts with the duty to preserve life? What safeguards exist to prevent abuse? And who is monitoring whether hospitals are truly prioritizing patient care over the lucrative transplant business?
These are questions every American should be asking, especially as they make decisions about organ donor status on their driver’s licenses. The system has changed dramatically, but few people understand just how much.
Let us know what you think, please share your thoughts in the comments below.